An effective COVID treatment the media continues to besmirch
08/05/2020 / By News Editors

On Friday, July 31, in a column ostensibly dealing with health care “misinformation,” Washington Post media critic Margaret Sullivan opened by lambasting “fringe doctors spouting dangerous falsehoods about hydroxychloroquine as a COVID-19 wonder cure.”
(Article by Steven Hatfill republished from RealClearPolitics.com)
Actually, it was Sullivan who was spouting dangerous falsehoods about this drug, something the Washington Post and much of the rest of the media have been doing for months. On May 15, the Post offered a stark warning to any Americans who may have taken hope in a possible therapy for COVID-19. In the newspaper’s telling, there was nothing unambiguous about the science — or the politics — of hydroxychloroquine: “Drug promoted by Trump as coronavirus game-changer increasingly linked to deaths,” blared the headline. Written by three Post staff writers, the story asserted that the effectiveness of hydroxychloroquine in treating COVID-19 is scant and that the drug is inherently unsafe. This claim is nonsense.
Biased against the use of hydroxychloroquine for COVID-19 — and the Washington Post is hardly alone — the paper described an April 21, 2020, drug study on U.S. Veterans Affairs patients hospitalized with the illness. It found a high death rate in patients taking the drug hydroxychloroquine. But this was a flawed study with a small sample, the main flaw being that the drug was given to the sickest patients who were already dying because of their age and severe pre-existing conditions. This study was quickly debunked. It had been posted on a non-peer-reviewed medical archive that specifically warns that studies posted on its website should not be reported in the media as established information.
Yet, the Post and countless other news outlets did just the opposite, making repeated claims that hydroxychloroquine was ineffective and caused serious cardiac problems. Nowhere was there any mention of the fact that COVID-19 damages the heart during infection, sometimes causing irregular and sometimes fatal heart rhythms in patients not taking the drug.
To a media unrelentingly hostile to Donald Trump, this meant that the president could be portrayed as recklessly promoting the use of a “dangerous” drug. Ignoring the refutation of the VA study in its May 15 article, the Washington Post cited a Brazil study published on April 24 in which a COVID trial using chloroquine (a related but different drug than hydroxychloroquine) was stopped because 11 patients treated with it died. The reporters never mentioned another problem with that study: The Brazilian doctors were giving their patients lethal cumulative doses of the drug.
On and on it has gone since then, in a circle of self-reinforcing commentary. Following the news that Trump was taking the drug himself, opinion hosts on cable news channels launched continual attacks on both hydroxychloroquine and the president. “This will kill you!” Fox News Channel’s Neil Cavuto exclaimed. “The president of the United States just acknowledge that he is taking hydroxychloroquine, a drug that [was] meant really to treat malaria and lupus.”
Washington Post reporters Ariana Cha and Laurie McGinley were back again on May 22, with a new article shouting out the new supposed news: “Antimalarial drug touted by President Trump is linked to increased risk of death in coronavirus patients, study says.” The media uproar this time was based on a large study just published in the Lancet. There was just one problem. The Lancet paper was fraudulent and it was quickly retracted.
However, the damage from the biased media storm was done and it was long-lasting. Continuing patient enrollment needed for early-use clinical trials of hydroxychloroquine dried up within a week. Patients were afraid to take the drug, doctors became afraid to prescribe it, pharmacies refused to fill prescriptions, and in a rush of incompetent analysis and non-existent senior leadership, the FDA revoked its Emergency Use Authorization for the drug.
So what is the real story on hydroxychloroquine? Here, briefly, is what we know:
When the COVID-19 pandemic began, a search was made for suitable antiviral therapies to use as treatment until a vaccine could be produced. One drug, hydroxychloroquine, was found to be the most effective and safe for use against the virus. Federal funds were used for clinical trials of it, but there was no guidance from Dr. Anthony Fauci or the NIH Treatment Guidelines Panel on what role the drug would play in the national pandemic response. Fauci seemed to be unaware that there actually was a national pandemic plan for respiratory viruses.
Following a careful regimen developed by doctors in France, some knowledgeable practicing U.S. physicians began prescribing hydroxychloroquine to patients still in the early phase of COVID infection. Its effects seemed dramatic. Patients still became sick, but for the most part they avoided hospitalization. In contrast — and in error — the NIH-funded studies somehow became focused on giving hydroxychloroquine to late-presenting hospitalized patients. This was in spite of the fact that unlike the drug’s early use in ambulatory patients, there was no real data to support the drug’s use in more severe hospitalized patients.
By April, it was clear that roughly seven days from the time of the first onset of symptoms, a COVID-19 infection could sometimes progress into a more radical late phase of severe disease with inflammation of the blood vessels in the body and immune system over-reactions. Many patients developed blood clots in their lungs and needed mechanical ventilation. Some needed kidney dialysis. In light of this pathological carnage, no antiviral drug could be expected to show much of an effect during this severe second stage of COVID.
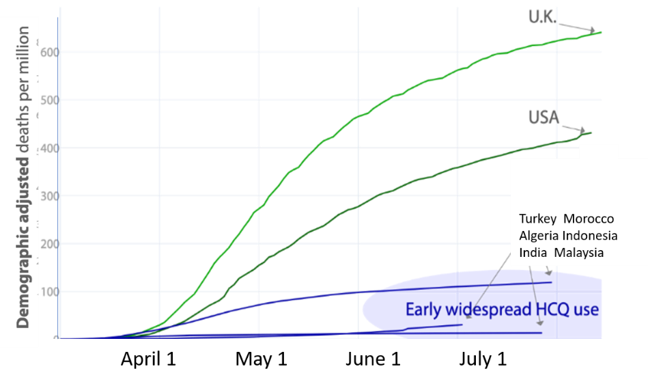
On April 6, 2020, an international team of medical experts published an extensive study of hydroxychloroquine in more than 130,000 patients with connective tissue disorders. They reaffirmed that hydroxychloroquine was a safe drug with no serious side effects. The drug could safely be given to pregnant women and breast-feeding mothers. Consequently, countries such as China, Turkey, South Korea, India, Morocco, Algeria, and others began to use hydroxychloroquine widely and early in their national pandemic response. Doctors overseas were safely prescribing the drug based on clinical signs and symptoms because widespread testing was not available.
However, the NIH promoted a much different strategy for the United States. The “Fauci Strategy” was to keep early infected patients quarantined at home without treatment until they developed a shortness of breath and had to be admitted to a hospital. Then they would they be given hydroxychloroquine. The Food and Drug Administration cluelessly agreed to this doctrine and it stated in its hydroxychloroquine Emergency Use Authorization (EUA) that “hospitalized patients were likely to have a greater prospect of benefit (compared to ambulatory patients with mild illness).”
In reality just the opposite was true. This was a tragic mistake by Fauci and FDA Commissioner Dr. Stephen Hahn and it was a mistake that would cost the lives of thousands of Americans in the days to come.
At the same time, accumulating data showed remarkable results if hydroxychloroquine were given to patients early, during a seven-day window from the time of first symptom onset. If given during this window, most infections did not progress into the severe, lethal second stage of the disease. Patients still got sick, but they avoided hospitalization or the later transfer to an intensive care unit. In mid-April a high-level memo was sent to the FDA alerting them to the fact that the best use for hydroxychloroquine was for its early use in still ambulatory COVID patients. These patients were quarantined at home but were not short of breath and did not yet require supplemental oxygen and hospitalization.
Failing to understand that COVID-19 could be a two-stage disease process, the FDA ignored the memo and, as previously mentioned, it withdrew its EUA for hydroxychloroquine based on flawed studies and clinical trials that were applicable only to late-stage COVID patients.
By now, however, some countries had already implemented early, aggressive, outpatient community treatment with hydroxychloroquine and within weeks were able to minimize their COVID deaths and bring their national pandemic under some degree of control.
In further contrast, countries that started out with the “Fauci-Hahn Doctrine” and then later shifted their policy towards aggressive outpatient hydroxychloroquine use, after a brief lag period also saw a stunning rapid reduction in COVID mortality and hospital admissions.
Finally, several nations that had started using an aggressive early-use outpatient policy for hydroxychloroquine, including France and Switzerland, stopped this practice when the WHO temporarily withdrew its support for the drug. Five days after the publication of the fake Lancet study and the resulting media onslaught, Swiss politicians banned hydroxychloroquine use in the country from May 27 until June 11, when it was quickly reinstated.

The consequences of suddenly stopping hydroxychloroquine can be seen by examining a graph of the Case Fatality Ratio Index (nrCFR) for Switzerland. This is derived by dividing the number of daily new COVID fatalities by the new cases resolved over a period with a seven-day moving average. Looking at the evolution curve of the CFR it can be seen that during the weeks preceding the ban on hydroxychloroquine, the nrCFR index fluctuated between 3% and 5%.
Following a lag of 13 days after stopping outpatient hydroxychloroquine use, the country’s COVID-19 deaths increased four-fold and the nrCFR index stayed elevated at the highest level it had been since early in the COVID pandemic, oscillating at over 10%-15%. Early outpatient hydroxychloroquine was restarted June 11 but the four-fold “wave of excess lethality” lasted until June 22, after which the nrCFR rapidly returned to its background value.
Here in our country, Fauci continued to ignore the ever accumulating and remarkable early-use data on hydroxychloroquine and he became focused on a new antiviral compound named remdesivir. This was an experimental drug that had to be given intravenously every day for five days. It was never suitable for major widespread outpatient or at-home use as part of a national pandemic plan. We now know now that remdesivir has no effect on overall COVID patient mortality and it costs thousands of dollars per patient.
Hydroxychloroquine, by contrast, costs 60 cents a tablet, it can be taken at home, it fits in with the national pandemic plan for respiratory viruses, and a course of therapy simply requires swallowing three tablets in the first 24 hours followed by one tablet every 12 hours for five days.
There are now 53 studies that show positive results of hydroxychloroquine in COVID infections. There are 14 global studies that show neutral or negative results — and 10 of them were of patients in very late stages of COVID-19, where no antiviral drug can be expected to have much effect. Of the remaining four studies, two come from the same University of Minnesota author. The other two are from the faulty Brazil paper, which should be retracted, and the fake Lancet paper, which was.
Millions of people are taking or have taken hydroxychloroquine in nations that have managed to get their national pandemic under some degree of control. Two recent, large, early-use clinical trials have been conducted by the Henry Ford Health System and at Mount Sinai showing a 51% and 47% lower mortality, respectively, in hospitalized patients given hydroxychloroquine. A recent study from Spain published on July 29, two days before Margaret Sullivan’s strafing of “fringe doctors,” shows a 66% reduction in COVID mortality in patients taking hydroxychloroquine. No serious side effects were reported in these studies and no epidemic of heartbeat abnormalities.
This is ground-shaking news. Why is it not being widely reported? Why is the American media trying to run the U.S. pandemic response with its own misinformation?
Read more at: RealClearPolitics.com
Tagged Under: Big Pharma, Censorship, coronavirus, Cover-Up, COVID, fake news, hydroxychloroquine, infections, mainstream media, outbreak, pandemic, rigged, truth, vaccine
RECENT NEWS & ARTICLES